Dr. Ramirez attended medical school at the Universidad Autonoma of Guadalajara School of Medicine in Guadalajara Mexico. Dr. Ramirez performed his Neurosurgery training at the National Institute of Neurology and Neurosurgery in Mexico City

Pituitary surgery is an operation mainly performed to treat tumors on or near the pituitary gland. The pituitary is a small gland at the base of the brain, approximately three inches behind the bridge of the nose. It produces multiple hormones, which control different systems throughout the body. Pituitary surgery can be performed with no visible incisions.
The type of approach largely depends on the location and size of the pituitary tumor. A neurosurgeon can access and remove these tumors by operating through either the top of the skull or through the nose.
The most common approach is operating through the sphenoid sinus in the nose, an approach called transsphenoidal surgery. To perform transsphenoidal surgery, a neurosurgeon travels through the nostril or the gums, without an incision in the skin. This is often referred to as microscopic transsphenoidal surgery or endoscopic endonasal surgery.
If the tumor is unusually large or infiltrating deep into the brain, a neurosurgeon may choose instead to operate through the skull by performing a craniotomy. In this procedure, a neurosurgeon makes an incision on the scalp and then removes part of the skull to gain access to the brain.
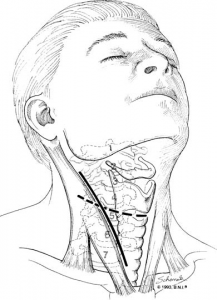
Figure 1. Approach for cervical discectomy and fusion
A tumor that grows in the pituitary gland is called an adenoma. Tumors of the pituitary gland are classified as functional or nonfunctional.
These tumors secrete abnormal levels of hormones and interfere with the normal hormonal regulation process. These tumors behave according to the cell of origin and are named for the specific hormone they produce. For example, if a tumor originates in a prolactin-producing cell, a prolactin-secreting tumor (prolactinoma) will result.
These tumors do not secrete hormones. Instead, they grow until the big size cause symptoms such as headache, vision loss, vomiting, and more symptoms. Large tumors may compress the optic nerves and invade the cavernous sinuses, which house the carotid arteries and some cranial nerves.
Symptoms of a pituitary tumor may vary depending on its size and hormone secretion function; however, many are asymptomatic. About 25 % are nonfunctional tumors; 75 are functional. Of hormonally active adenomas, about 50 % secrete prolactin, 20 % secrete growth hormone, 20 % secrete adrenocorticotropic hormone, and 10 % secrete multiple hormones
The most common indication for surgery is pituitary tumors. Also, different diseases, especially another type of tumors located in the pituitary area can be treated by the same surgical principles of pituitary surgery.
This is the list of conditions treated with transsphenoidal surgery (microscopic or endoscopic):
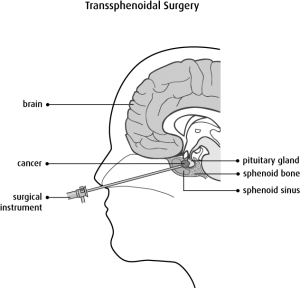
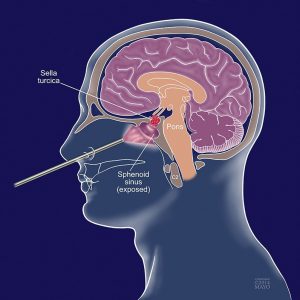
Figure 1. Microscopic transsphenopidal surgery
This is the most common way to remove pituitary tumors. Transsphenoidal means that the operation is done through the sphenoid sinus, a hollow space in the skull behind the nasal passages and below the brain. The back wall of the sinus covers the pituitary gland. To do this surgery, the neurosurgeon makes a small incision along the nasal septum ( or under the upper lip (above the teeth). To reach the pituitary, the surgeon opens the boney walls of the sphenoid sinus with small surgical chisels, drills, or other instruments depending on the thickness of the bone and sinus. Small tools and a microscope are used to remove the tumor (Figure 1).
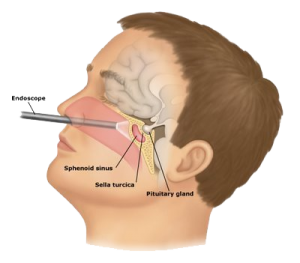
Figure 2. Endoscopic endonasal transsphenoidal surgery
Another approach is to use an endoscope, a thin fiber-optic tube with a tiny camera at the tip. This is a minimally invasive technique. In this way, the incision under the upper lip or along the nasal septum is not needed, because the endoscope allows the surgeon to see through a small incision that is made in the back of the nasal septum (Figure 2). The surgeon passes instruments through the nose and opens the sphenoid sinus to reach the pituitary gland and take out the tumor. Whether this technique can be used depends on the tumor’s position and the shape of the sphenoid sinus.
The transsphenoidal approach has many advantages. First, no part of the brain is touched during the surgery, so the chance of damaging the brain is very low. There may be fewer side effects, and there’s also no visible scar. But this surgery may take longer, and it is hard to take out large tumors this way.
When this surgery is done by an experienced neurosurgeon and the tumor is small, the cure rates are high. If the tumor is large or has grown into the nearby structures (such as nerves, brain tissue, or the tissues covering the brain) the chances for a cure are lower and the chance of damaging nearby brain tissue, nerves, and blood vessels is higher.
For larger or more complicated pituitary tumors, a craniotomy may be needed. In this approach, the surgeon operates through an opening in the front of the skull, off to one side. The surgeon has to work carefully beneath and between the lobes of the brain o reach the tumor (Figure 3). Craniotomy has a higher chance of brain injury and other side effects than transsphenoidal surgery for small lesions, but it’s safer for large and complex lesions because the surgeon is better able to see and reach the tumor as well as nearby nerves and blood vessels.
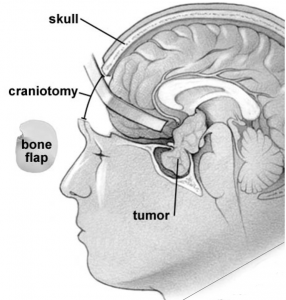
Figure 3. Craniotomy for pituitary tumor
Dr. Ramirez attended medical school at the Universidad Autonoma of Guadalajara School of Medicine in Guadalajara Mexico. Dr. Ramirez performed his Neurosurgery training at the National Institute of Neurology and Neurosurgery in Mexico City

Dr. Ramiro Pérez attended medical school at the University of Guadalajara School of Medicine in Guadalajara México. Dr. Pérez performed his Neurosurgery training in Centro Medico Siglo XXI IMSS and has been practicing his specialty for more than 13 years.

Dr. Nares attended medical school at the University of Aguascalientes, He is trained to perform anterior and lateral approaches to the spine from the cervical to the lumbar spine, as well as minimally invasive surgery.

Dr. Luis Robles has been practicing neurosurgery specialty for 20 years. Dr. Robles is academically active, he participates as a section editor in the World Neurosurgery journal and he has published several articles in different neurosurgery international journals.